The CMS Contract Year 2027 Final Rule reshapes Medicare lead-gen timing economics. The 48-hour Scope of Appointment hold is gone, the 12-hour educational-to-marketing gap is gone, the TPMO disclaimer moves off the 60-second clock, and the July 31, 2026 HPMS deadline puts a hard line under carrier compensation reporting.
A marketing rule rollback inside a four-month window
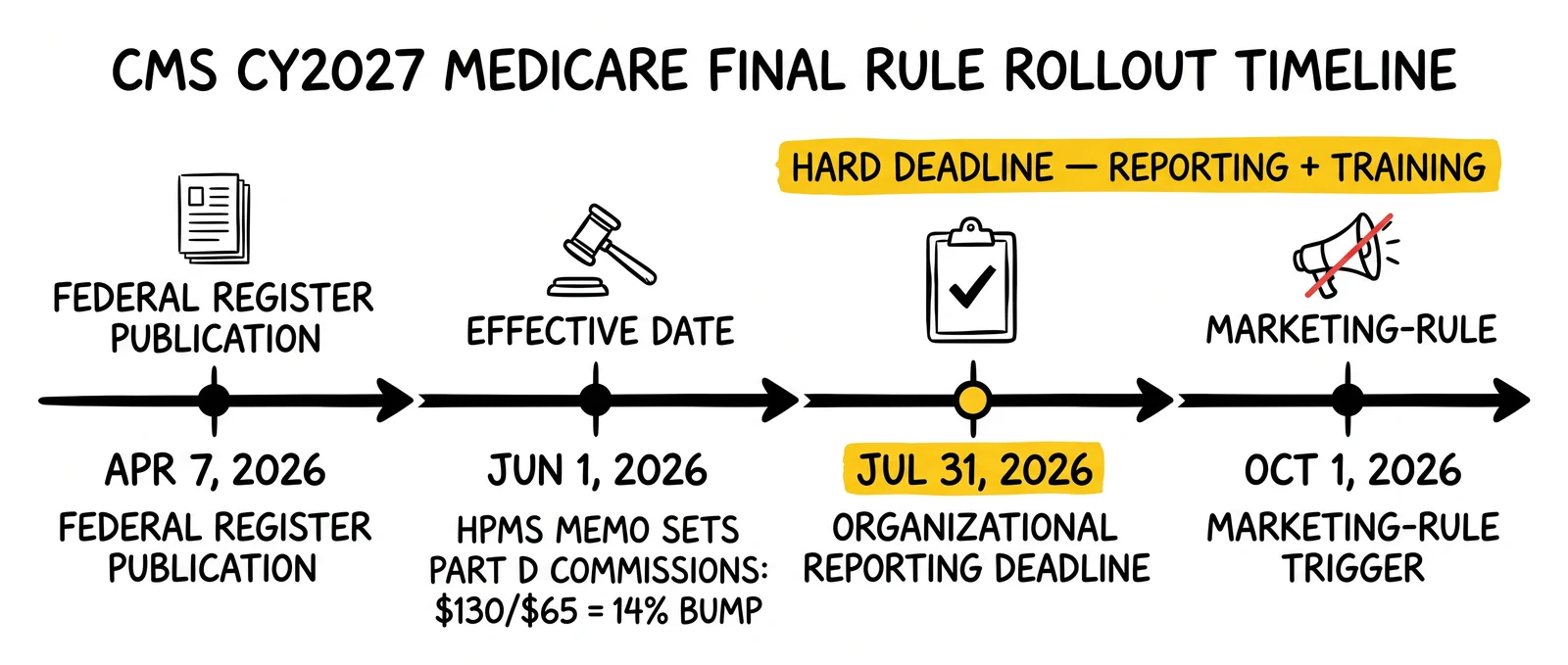
The Centers for Medicare and Medicaid Services published the Contract Year 2027 Medicare Advantage and Part D Final Rule in the Federal Register on April 7, 2026 (CMS-4208-F3 and CMS-4212-F, RIN 0938-AV40, Federal Register document 2026-06600). The rule carries a regulatory effective date of June 1, 2026. The marketing and communications provisions – the part of the rule that most directly resets Medicare lead-gen operations – apply to all CY2027 marketing and communications activity beginning October 1, 2026. Coverage under the rule runs through plan year 2027 starting January 1, 2027.
The 2027 Rate Announcement landed the same day. CMS finalized a 2.48 percent average payment increase to MA plans for CY2027, more than $13 billion in additional plan payments versus 2026, with a 4.98 percent effective revenue change after accounting for risk-score trend. That payment increase exceeded the 0.09 percent signaled in the November 28, 2025 Advance Notice and came in well below the 5.06 percent finalized for CY2026.
The plan-revenue uplift is the part of the picture that funds the second half of the change set. On June 1, 2026, CMS issued the Health Plan Management System memo titled Agent Broker Compensation and Training and Testing Requirements CY2027. The memo raised the national maximum Medicare Advantage initial commission from $694 to $725 per member per year, the national renewal from $347 to $363, and the Part D initial commission from $114 to $130 with renewals at $65 – a 14 percent year-over-year increase on both Part D figures. The same memo set a July 31, 2026 hard deadline for MA organizations, Part D sponsors, and Cost Plan organizations to submit and attest to agent and broker compensation data in HPMS for plan year 2027.
Three months of operator runway sits between the June 1 effective date and the October 1 marketing-rule trigger. AEP 2027 opens October 15, 2026 – eight days after the marketing rollback takes effect. The compression matters. Operators that read the rollback as a relaxation of compliance load are reading it wrong; the rule consolidates the conversion timeline and increases the volume of marketing activity per unit of compliance documentation. The audit trail for each lead-to-enrollment funnel will run shorter but denser.
The 48-hour SOA waiting period is gone
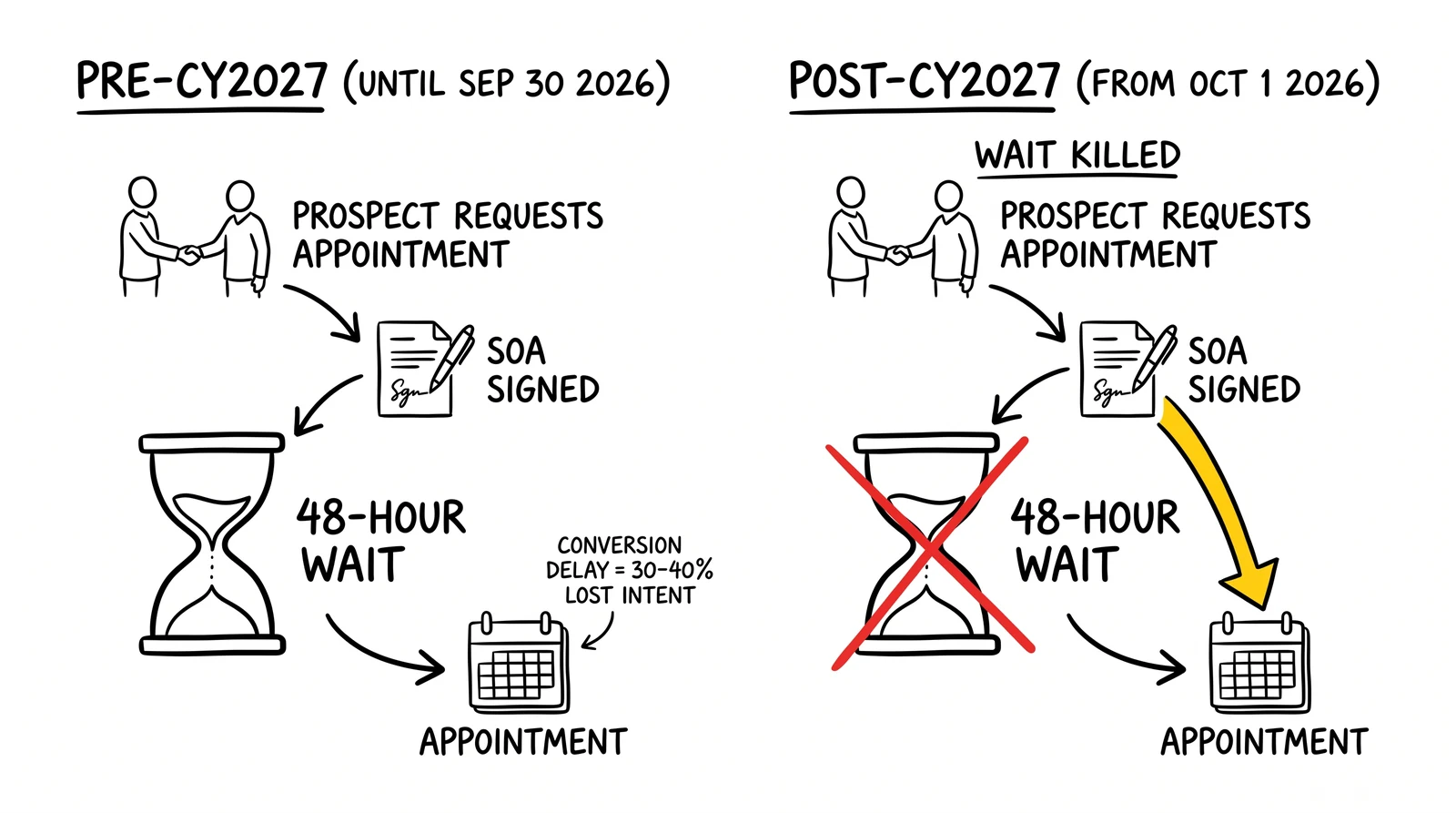
The biggest single timing change in the rule is the elimination of the 48-hour Scope of Appointment waiting period codified at 42 CFR sections 422.2264(c)(3) and 423.2264(c)(3). Beginning October 1, 2026, an agent or broker can collect a signed Scope of Appointment from a Medicare-eligible beneficiary and immediately proceed to a personal marketing appointment in the same call, the same meeting, or the same day. CMS framed the change as the removal of an unnecessary barrier to beneficiary access to MA and Part D information.
The advance-notice requirement remains. CMS did not eliminate the SOA itself – only the cooling-off window between SOA capture and the marketing discussion. The agent or broker still has to obtain an SOA documenting which plan types the conversation will cover. What’s gone is the requirement that the beneficiary sit on the documentation for two days before the agent can talk about plans.
Inbound calls were already exempt from the 48-hour wait. The change matters most for three flows where Medicare lead-gen operators have been working around the prior rule:
Outbound dialer flows. Outbound TPMO call centers that contact beneficiaries on documented PEWC consent and need an SOA before plan discussion previously had to scheduled a callback at least 48 hours later. The lead-to-marketing-discussion gap embedded in the prior rule pushed conversion timing into a multi-touch sequence that suffered the well-documented decay curve on Medicare lead intent. Same-call SOA plus same-call plan discussion compresses that into a single touch.
Educational event funnels. Field agents holding educational events under the CY2023 rules had to gather attendee contact information, schedule a follow-up at least 48 hours out, and conduct the marketing appointment separately. The CY2027 rule allows the SOA to be collected at the educational event and the marketing appointment to occur immediately afterward. (See the 12-hour gap discussion below.)
Internet lead handoffs. Lead-gen operators that delivered Medicare leads to downstream agents via ping-post or live-transfer infrastructure had to architect a multi-touch sequence where the consumer received an SOA, completed it, returned it, then received an outbound marketing call no earlier than 48 hours later. The single-touch path is now compliant.
The operator question is not whether to use the same-call flow but how to instrument it. The SOA documentation requirement does not disappear; it gets faster. Operators who replace the 48-hour hold with a same-call workflow need timestamp evidence that the SOA was captured before the plan-benefits discussion began. The compliance posture is now a sequence-of-events audit rather than a calendar audit.
What inbound call centers should change
Inbound contact centers historically managed the SOA at the front of the call. The change to disclaimer timing – discussed in the next section – affects inbound call flows more than the SOA change does. The inbound posture from CMS on same-call SOA and marketing has not changed in substance; the change to outbound and follow-up flows is what closes the prior gap.
For inbound centers running on dialers and call-routing platforms like Convoso, Five9, or Genesys, the script-engine changes are limited to disclaimer placement. The SOA capture interface and the same-call marketing flow already existed in most CY2023-compliant scripts.
The TPMO disclaimer moves off the 60-second clock
Effective October 1, 2026, the TPMO disclaimer no longer needs to be read within the first 60 seconds of a sales or marketing call. The new trigger is delivery before any discussion of plan benefits. CMS preserved the substantive disclosure content – the disclaimer still has to communicate that the TPMO does not offer every plan available in the area and direct beneficiaries to 1-800-MEDICARE or Medicare.gov – but removed the State Health Insurance Assistance Program reference and adjusted the timing.
Three operator implications:
General statements about plan categories don’t trigger the disclaimer. CMS clarified that statements such as “most Medicare Advantage plans include dental coverage” or “many Part D plans offer mail-order pharmacy” are not plan-specific benefit discussions and do not require the disclaimer. Educational and orientation conversations can occur for longer than 60 seconds before the disclaimer becomes required.
Call scripts written for the 60-second rule need re-engineering. Outbound and inbound script writers built the prior compliance posture around a hard 60-second timer. The new trigger is conversational – a benefit-specific discussion. Scripts need a logic gate that identifies the point at which the agent moves from general orientation into specific plan benefits and triggers the disclaimer at that boundary. Call-center QA workflows that automatically flagged any call without disclaimer audio in the first 60 seconds will produce false positives under the new rule.
The State Health Insurance Assistance Program reference comes out. CMS removed the SHIP reference from the required disclaimer language while preserving Medicare.gov and 1-800-MEDICARE references. Operators with hard-coded script libraries should pull the SHIP language out by October 1, 2026 because retaining superseded disclosure language can itself produce a misleading-communications exposure under the general prohibition that survives the rule.
Recording retention drops from 10 years to 6
The CY2027 rule reduces the retention period for sales and marketing call recordings from 10 years to 6 years. The first 3 years require full audio retention. Years 4 through 6 can be retained as audio or as written transcripts. Calls that result in a plan enrollment continue to require a 10-year retention period under the enrollment-record rules – the 6-year reduction is a sales/marketing retention change, not an enrollment-record retention change.
The storage-cost impact for high-volume Medicare TPMOs is real. A 5,000-seat call center generating 100,000 hours of recorded calls per month at 64 kbps Opus encoding produces roughly 2.7 TB per month, 32 TB per year, 320 TB across 10 years. Cutting the retention to 6 years and allowing transcript-only storage for years 4 through 6 cuts the long-tail storage footprint by approximately 60 percent depending on transcript compression. AWS S3 Glacier Deep Archive pricing at $0.00099 per GB-month produces a per-organization annual savings in the five-figure range; for FMOs and large TPMOs with multi-petabyte archives, the savings move into the six figures.
The harder operational question is reconciling the dual retention requirement. The same call may carry both classifications. A marketing-and-enrollment call that completes an enrollment requires 10-year retention. The same call sequence that ends without enrollment requires 6-year retention. Call-archive systems need a classification field driven by the outcome of the call, not the type of the call.
Educational events and the 12-hour gap kill
The CY2027 rule eliminates the 12-hour prohibition between educational events and marketing events held at the same location, as long as beneficiaries receive notification of the transition and an opportunity to leave before plan-specific marketing begins. CMS also confirmed that delivery and collection of Scope of Appointment forms at educational events does not constitute a sales or marketing activity.
The combination compresses the educational-to-enrollment workflow into a single-venue, same-day flow:
- An agent holds an educational event at a community center.
- Attendees who opt in receive an SOA at the educational event itself.
- The educational event ends, attendees are notified that a marketing presentation will follow, those who choose to leave do so, and those who remain attend the marketing presentation in the same venue without any waiting period.
Field-agent training that built around the 12-hour gap and the no-SOA-at-educational-event rules needs a full rewrite for the October 1, 2026 effective date. The CY2023 rules forced agents to schedule two events, two venues, and a 12-hour gap; the CY2027 rules allow one event, one venue, one continuous workflow with a documented opt-out moment in the middle.
The compliance documentation focus shifts to the opt-out moment. Operators need recorded evidence – minutes, attendance logs, an audible announcement on the venue’s recording – that beneficiaries received the transition notice and had the opportunity to leave. The 12-hour gap functioned as a structural protection that compliance teams could audit calendar-by-calendar. The new structure requires a transcript-level audit.
Carrier participation, FMO compensation, and the same-venue economics
The same-venue flow changes the unit economics of educational events for FMOs and IMOs that subsidize agent activity. The cost-per-enrollment math improves when one event produces both education and enrollment opportunity without a second-venue setup. Educational events have historically been a top-of-funnel cost center subsidized by enrollment commissions – same-venue marketing means a single fixed cost can be amortized across both touch points. The CY2027 commission bumps further improve the math.
The FMO-side question is which agents the rule helps most. Captive agents already operating in carrier facilities can run same-venue flows. Independent agents working through community-center rentals or coffee-shop educational sessions previously had to build the 12-hour gap into the venue rental schedule, which raised the marginal cost of educational outreach. The CY2027 rule removes that friction.
The June 1 HPMS memo and the July 31, 2026 hard deadline
The June 1, 2026 CMS HPMS memo titled Agent Broker Compensation and Training and Testing Requirements CY2027 set the maximum Fair Market Value commission rates for plan year 2027 and the operational reporting deadline.
The Medicare Advantage national maximums increased from CY2026 levels:
| Plan Year | National MA Initial | National MA Renewal | CT / PA / DC Initial | CT / PA / DC Renewal | CA / NJ Initial | CA / NJ Renewal | PR / USVI Initial | PR / USVI Renewal |
|---|---|---|---|---|---|---|---|---|
| 2026 | $694 | $347 | $781 | $391 | $864 | $432 | $474 | $237 |
| 2027 | $725 | $363 | $816 | $408 | $902 | $451 | $495 | $248 |
The Part D national maximums rose more steeply:
| Plan Year | Part D Initial | Part D Renewal |
|---|---|---|
| 2026 | $114 | $57 |
| 2027 | $130 | $65 |
The national MA initial commission increased 4.5 percent. The national MA renewal increased 4.6 percent. The Part D initial and renewal increased 14 percent each. Regional rates in California and New Jersey reach $902 initial – nearly 25 percent above the national maximum. The maximums represent the cap on what plan sponsors may pay; commission payments remain at carrier discretion within the Fair Market Value ceiling. Carriers may pay all, some, or none of the maximum.
The hard deadline is July 31, 2026 at 11:59 PM Eastern Time. By that timestamp, every MA organization, Part D sponsor, and Cost Plan organization must submit and attest in the HPMS Marketing Module to the agent and broker compensation data for plan year 2027. The submission must specify:
- Whether the organization will use employed agents, captive agents, independent agents, or some combination
- The specific rates or range of rates the organization will pay independent agents and brokers
- Confirmation that the compensation does not exceed the Fair Market Value ceilings
Organizations that fail to submit and attest by the deadline are out of compliance with CMS requirements for plan year 2027. The submission window opened June 1, 2026 and runs through the cutoff. FMOs and IMOs do not file directly – the obligation sits with the contracting plan sponsor. Independent agents and brokers contracted through multiple carriers need to confirm that each carrier they enroll under has filed and attested by July 31.
What the commission bump means for AEP economics
The 14 percent Part D commission bump reverses a multi-year trend of stagnant Part D economics. The Part D initial commission climbed from $100 in CY2024 to $114 in CY2026 to $130 in CY2027 – with renewal pacing roughly half the initial throughout. The Part D vertical, which had been an afterthought in many FMO compensation conversations, becomes meaningfully more profitable per enrollment in 2027.
The MA national increase of 4.5 percent on initial commissions is more modest in percentage terms but represents the largest absolute dollar increase ever to the national MA maximum – $31 per member per year per initial enrollment, compounding across renewal years. For a national TPMO running 100,000 enrollments per AEP, the dollar-per-enrollment ceiling moves up by $3.1 million in initial commission capacity alone.
Regional rate differentials matter for FMO panel composition. An agent panel concentrated in California, New Jersey, Connecticut, Pennsylvania, or DC has access to higher absolute commissions ($816 to $902 initial) and should price marketing spend accordingly. National FMOs running uniform CPL targets across all geographies leave commission dollars on the table. The CY2027 maximum-cap structure rewards FMOs that geo-target marketing spend against the regional commission curve.
Star Ratings, Part D redesign, and the rest of the rule
The CY2027 Final Rule made three additional changes that affect Medicare lead-gen operations more indirectly but that operators should understand.
Star Ratings. CMS removed 11 measures from the Star Ratings calculations, primarily administrative or process-based, with most reductions effective beginning with the 2029 Star Ratings measurement period and a smaller subset effective 2028. The rule also added one depression-screening measure. Star Ratings drive plan-enrollment volume because plans rated 4 stars or above get the rebate-and-bonus uplift. Lead-gen operators selling against high-rated plans should expect Star Ratings recalculation effects on plan supply starting in late 2027.
Part D redesign. The annual out-of-pocket threshold for Part D is set at $2,100 for CY2026 and indexed annually thereafter. The benefit restructures into three phases – deductible, initial coverage, and catastrophic – with manufacturers facing civil penalties for non-compliance with discount requirements. The Part D cost-protection improvements increase the consumer-side incentive to enroll in stand-alone Part D plans or MA-PD plans, which feeds the Part D lead pipeline directly.
Marketing rollback details. The prohibition on the use of superlatives in marketing materials without supporting documentation was removed, although the general prohibition on misleading communications survives. CMS also eliminated the notice-of-language-assistance requirement and three health-equity requirements. The general direction of the marketing rollback is consistent: CMS reduced the procedural compliance burden while preserving the substantive prohibition on misleading or inaccurate communications.
The marketing-rollback survivors – the substantive prohibitions that remain – are the audit-trail focal points for operators. State attorney-general enforcement under unfair-and-deceptive-acts-and-practices statutes operates independently of the CMS rule rollbacks. An MA marketing claim that survives CMS scrutiny under the new looser rules can still draw state AG enforcement if the claim is misleading. The CY2027 rollback is a federal-floor relaxation, not a state-ceiling preemption.
What the rule does not change – and the consent-sharing trap
Three CMS rules survived the CY2027 rollback intact, and operators reading the rollback summary as a broad compliance relaxation risk hitting the surviving rules.
One-to-one consent for beneficiary data sharing remains. The CMS one-to-one consent requirement for TPMOs sharing beneficiary data with other TPMOs or plan sponsors was not modified in the CY2027 Final Rule. Beneficiary contact information still cannot be shared with another entity without prior written consent that specifically identifies the recipient. The Federal Communications Commission’s separate one-to-one consent rule for TCPA marketing calls was vacated by the Eleventh Circuit in January 2025, but that vacatur operates on FCC TCPA authority and does not affect the CMS consent-sharing rule for Medicare beneficiary data – see the deeper coverage of Medicare marketing compliance. Operators that confused the FCC vacatur for a Medicare consent-sharing rollback have been working under a false posture.
Civil Monetary Penalties stay. CMS retains the authority to impose Civil Monetary Penalties exceeding $100,000 per violation for marketing rule violations and to terminate Medicare participation entirely for serious or repeated violations. The CY2027 rule changes the timing and content of certain procedural requirements; it does not reduce the penalty exposure for violating those requirements.
TPMO classification still functional, not definitional. Any entity performing lead-generation, marketing, sales, or enrollment functions for Medicare Advantage or Part D plans remains a TPMO under CMS rules regardless of self-description. Operators identifying themselves as “lead generators” rather than “TPMOs” remain subject to TPMO rules. The CY2027 rule did not narrow the TPMO definition.
The October 1, 2026 trigger affects how Medicare leads can be timed, not whether they can be sold to multiple buyers without specific consent. The one-to-one consent rule for Medicare lead generation under AEP and OEP economics still constrains lead distribution architecture.
Operator playbook: five actions before October 1, 2026
Five operational actions sit inside the window between June 25 and October 1, 2026. The list is sequenced by operational dependency, not by importance.
1. Confirm the carrier filed by July 31, 2026. Every independent agent and broker contracted under one or more MA organizations, Part D sponsors, or Cost Plan organizations needs to verify the contracting carrier filed and attested the HPMS Marketing Module agent-and-broker compensation data by 11:59 PM Eastern Time on July 31, 2026. The contracting carrier is the responsible filer; agents are downstream. But agents working under a non-filing carrier are agents of a non-compliant organization, which raises the contracting-relationship risk profile.
2. Rewrite outbound and inbound call scripts for the disclaimer-before-benefits trigger. Call-script libraries built around the 60-second TPMO disclaimer timing need a logic gate identifying when the conversation moves from general orientation into plan-specific benefit discussion. The transition triggers the disclaimer. Scripts that hard-code the disclaimer at the front of every call will work under the new rule but will produce a longer-than-needed disclaimer-first call structure that hurts conversion.
3. Retool lead-routing workflow for same-call SOA plus same-call marketing. Lead-gen operators delivering Medicare leads via ping-post or live-transfer can drop the 48-hour scheduled-callback step. The post-SOA marketing call can occur in the same touch. Routing systems that enforced the 48-hour gap as a compliance lockout need to be modified to allow same-touch progression while preserving the timestamp audit trail showing SOA capture before plan-benefit discussion.
4. Retrain field agents on educational-event flow with SOA collection and same-venue marketing. Field-agent training built around the CY2023 12-hour gap and the no-SOA-at-educational-event rules is obsolete. Educational events can now include SOA collection and direct-transition marketing presentations at the same venue. The opt-out moment between educational and marketing becomes the compliance focal point – operators need documented evidence that the transition was announced and that attendees who chose to leave were able to.
5. Reconcile the 6-year sales/marketing recording retention against the 10-year enrollment retention. Call-archive systems need an outcome-driven classification field that distinguishes calls resulting in enrollment (10-year retention) from sales/marketing calls without enrollment (6-year retention, with audio-only for first 3 years and audio-or-transcript for years 4 through 6). Archives that uniformly applied the 10-year retention to all sales and marketing calls will carry unnecessary storage cost; archives that drop the 10-year retention for enrollment-positive calls will violate CMS enrollment-record rules.
The Medicare vertical has spent the last three years compounding compliance debt against the CY2023 and CY2024 final rules. The CY2027 rule resets that compliance baseline. Operators that treat the rollback as a holiday rather than a re-engineering deadline will lose AEP 2027 to operators that retooled.
Key Takeaways
- The CMS CY2027 Final Rule published April 7, 2026 carries a June 1, 2026 regulatory effective date and an October 1, 2026 trigger for marketing and communications provisions; coverage applies to plan year 2027 starting January 1, 2027.
- The 48-hour Scope of Appointment waiting period codified at 42 CFR sections 422.2264(c)(3) and 423.2264(c)(3) is eliminated; same-call or same-meeting SOA capture plus marketing is permitted beginning October 1, 2026.
- The 12-hour prohibition between educational and marketing events at the same venue is eliminated, with a documented opt-out moment becoming the compliance focal point.
- The TPMO disclaimer moves from a within-first-60-seconds trigger to a before-plan-benefits-discussion trigger; the SHIP reference is removed from required language.
- Marketing call recording retention drops from 10 years to 6 years, with full audio for the first 3 years and audio-or-transcript for years 4 through 6; enrollment records retain the 10-year requirement.
- The June 1, 2026 HPMS memo set 2027 national MA maximums at $725 initial and $363 renewal (4.5 and 4.6 percent increases) and Part D maximums at $130 initial and $65 renewal (14 percent increases).
- MA organizations, Part D sponsors, and Cost Plan organizations must submit and attest to agent and broker compensation data in the HPMS Marketing Module by 11:59 PM Eastern Time on July 31, 2026.
- The 2027 Rate Announcement finalized a 2.48 percent average MA payment increase and a 4.98 percent effective revenue change after risk-score trend – the funding source for the commission bumps.
- The one-to-one consent rule for Medicare beneficiary data sharing, the TPMO classification, and Civil Monetary Penalty authority all survive the CY2027 rollback intact.
Sources
- CMS Fact Sheet – Contract Year 2027 Medicare Advantage and Part D Final Rule (April 7, 2026)
- Federal Register – Medicare Program Contract Year 2027 Final Rule, Document 2026-06600 (April 6, 2026)
- CMS Press Release – CMS Finalizes 2027 Medicare Advantage and Part D Payment Policies (April 7, 2026)
- Holland and Knight – CMS Finalizes CY 2027 Medicare Advantage and Part D Rule (April 2026)
- Crowell and Moring – CMS Finalizes CY 2027 Medicare Advantage and Part D Rule: Key Implications for Plan Sponsors
- Ritter Insurance Marketing – 2027 Maximum Broker Commissions for Medicare Advantage and Medicare Part D
- Action Benefits – CMS Releases CY2027 Commissions for Medicare Advantage (June 2026)
- RISE Health – 7 Marketing Changes in the 2027 Medicare Advantage Final Rule
- Senior Benefit Services – The CMS 2027 Final Rule: Key Updates Every Medicare Agent Should Understand
- Home Health Care News – CMS Finalizes 2.48% Medicare Advantage Payment Increase For 2027